Childbirth Delivery Methods and Types
Every woman’s experience is unique but most mothers would honestly say, yes, childbirth is painful. However, it is short-lived, and there are many types and methods to effectively reduce the intensity of childbirth pain. There are many choices in childbirth. Women can choose the method that makes them most comfortable, and that makes sense for their personal and medical situation.
Medical technology has made childbirth a much safer experience over the past century for both mother and baby. Hospitals have responded to trends in childbirth, such as the need for a more home-like environment in the hospital. Many hospitals now offer comfortable maternity suites that convert into state of the art delivery rooms.
An easy birth and a perfectly executed birth plan are ideal. But we know that even the most carefully planned birth can take twists and turns. In those cases, it’s important to be prepared for alternative delivery methods.
Different Kinds of Childbirth and Delivery Methods
Vaginal Delivery
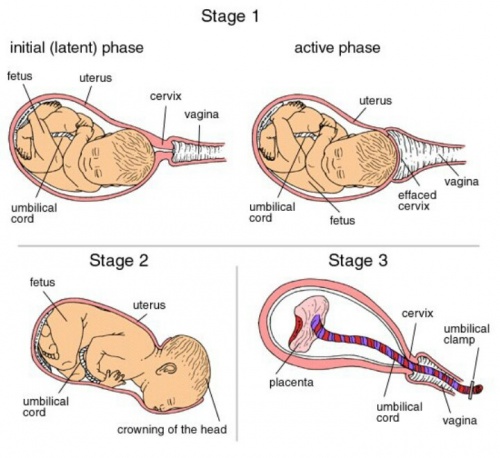
 In a vaginal birth, the baby is born through the birth canal. It’s hard to know when exactly you will go into labor, but most women give birth at around 38-41 weeks of pregnancy.
In a vaginal birth, the baby is born through the birth canal. It’s hard to know when exactly you will go into labor, but most women give birth at around 38-41 weeks of pregnancy.
A vaginal birth without medication benefits both mother and baby. The microbiome, or bacterial environment, is established by birth method. There is some research that suggests the development of the infant microbiome is associated with the likelihood of developing allergic diseases during childhood, but the association isn’t clear.
Benefits of vaginal delivery:
- Infants born vaginally tend to have fewer respiratory problems.
- Quicker recovery for the mother
- A lower rate of infection and a shorter hospital stay
Disadvantages of vaginal delivery
- Tearing of the perineum
- Sometimes, a vaginal birth may not be recommended for medical reasons.
Cesarean Section (C-Section) 
According to the Centers for Disease Control (CDC), about 1/3 of births are delivery by C-section, although rates are highly variable by hospital and region. The World Health Organization (WHO) says the rate of Cesarean deliveries should be about 10%-15%; the higher level is because of both elective Cesareans and overuse in the U.S.4 A C-section involves a horizontal incision across the lower abdomen through which the infant is delivered. The typical hospital stay is three days after a Cesarean to ensure the incision is healing. Full recovery can take 8 weeks. One advantage of a C-section is that the delivery date can be planned ahead of time. In certain circumstances, a C-section is scheduled in advance. In others, it’s done in response to an unforeseen complication.
Events that may require C-Section:
- Multiples (twins, triplets, etc)
- A very large baby
- Previous surgery, C-Sections, or other uterine conditions
- Baby is in breech (bottom first) or transverse (sideways) position
- Placenta previa (when the placenta is low in the uterus and covers the cervix)
- Fibroid or other large obstruction
- Medical conditions/complications
Water Birth
 A water birth means the mother goes through some or all of the stages of childbirth in a portable tub similar to a hot tub. The baby can be delivered underwater or the mother can get out of the water and deliver in a different position. Women chose water births because it can be more relaxing, and less painful to be in the water. Birthing tubs can be brought into the home for a home birth, and they are often found in birthing centers. Some hospitals may have birthing tubs as well.
A water birth means the mother goes through some or all of the stages of childbirth in a portable tub similar to a hot tub. The baby can be delivered underwater or the mother can get out of the water and deliver in a different position. Women chose water births because it can be more relaxing, and less painful to be in the water. Birthing tubs can be brought into the home for a home birth, and they are often found in birthing centers. Some hospitals may have birthing tubs as well.
Benefits of Water Birth:
- It allows the woman to move into a variety of positions that can feel more natural and less painful.
- The partner can also get into the tub with the mother to support the delivery.
Disadvantages of Water Birth:
- May increase the risk of infection, but as long as the water is fresh and clean, water births are not any riskier than non-water births.
- Unless the water birth takes place in a birth center with established tubs, there are logistics involved in setting up the tub and warming the water for a water birth.
- If the birth plan at home does not progress normally, it may require transport to a hospital.
Lamaze Method 
The Lamaze method is typically known for controlled breathing techniques but it includes a number of comfort strategies that can be used during labor. Breathing techniques increase relaxation and decrease the perception of pain. In addition to breathing, other information about preparing for childbirth is covered. Lamaze is taught in a series of classes attended by both the mother and her partner, when possible. The Lamaze method doesn’t explicitly encourage or discourage medications but seeks to educate women about their options so they can make a birth plan that suits their individual needs.
Benefits of the Lamaze Method:
- Lamaze training prepares the mother and her partner with a number of tools to use to get through labor and delivery naturally.
- The breathing and relaxation techniques reduce the perception of pain and keep labor moving smoothly.
- The Lamaze courses help the couple be prepared with what to expect over the first few days and weeks together.
Disadvantages of the Lamaze Method:
- Learning the Lamaze method takes time. The couple must plan ahead and attend classes starting in the second trimester of pregnancy.
Vacuum Extraction 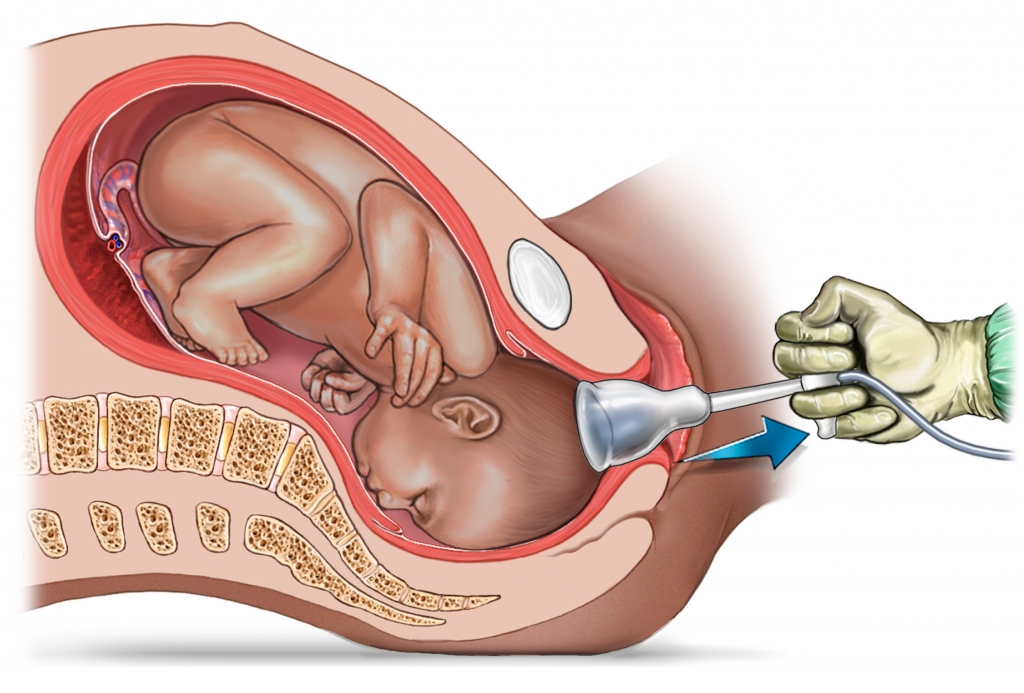
A vacuum extraction is a procedure sometimes done during the course of vaginal childbirth. A vacuum-assisted delivery involves attaching a soft cup to the head of the infant while it is in the birth canal and a hand-held pump is used to create suction to facilitate delivery.
- The advantage is that this assisted birth option has a lower risk than a C-section of prolonged fetal distress.
- The risks of this method include minor scalp injuries or more serious trauma or bleeding of the head.
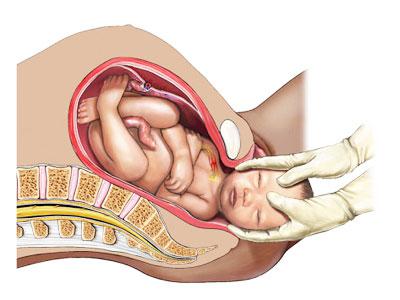
Forceps Delivery
A forceps delivery is a type of operative vaginal delivery. It’s sometimes needed in the course of vaginal childbirth. A forceps-assisted delivery means that curved instruments are used to facilitate the progress of the infant in the birth canal. Forceps cannot be used if the infant is breech, but it can be an option if the mother is too exhausted or if the infant has to be delivered more quickly than is naturally occurring.
The information, including but not limited to, text, graphics, images and other material contained on this website are for informational purposes only. The purpose of this website is to promote broad consumer understanding and knowledge of various health topics. It is not intended to be a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or another qualified healthcare provider with any questions you may have regarding a medical condition or treatment and before undertaking a new health care regimen, and never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Resources:
https://www.medicinenet.com/7_childbirth_and_delivery_methods/article.htm#what_is_a_water_birth