

What You Need To Know About Postpartum Depression
Postpartum depression (PPD), also called postnatal depression, is a type of mood disorder occurs in women soon after giving birth. It’s common for women to experience the “baby blues”, extreme sadness, low energy, anxiety, crying episodes, irritability, and changes in sleeping or eating patterns, following their baby’s birth. But some women, up to 1 in 7, experience a much more serious mood disorder.
The birth of a baby can trigger a jumble of powerful emotions, from excitement and joy to fear and anxiety. But it can also result in something you might not expect — depression.
 But some new moms experience a more severe, long-lasting form of depression known as postpartum depression. Rarely, an extreme mood disorder called postpartum psychosis also may develop after childbirth.
But some new moms experience a more severe, long-lasting form of depression known as postpartum depression. Rarely, an extreme mood disorder called postpartum psychosis also may develop after childbirth.
Postpartum depression isn’t a character flaw or a weakness. Sometimes it’s simply a complication of giving birth. If you have postpartum depression, prompt treatment can help you manage your symptoms — and enjoy your baby.
Here’s what you need to know about this common, yet entirely treatable, condition.
When does it occur?
Your recovering body may be vulnerable to certain infections after you have a baby. Some postpartum infections actually begin brewing during labor, though they often don’t become apparent for days – or even weeks – after delivery. Symptoms usually develop within the first few weeks after giving birth but may begin later — up to six months after birth.
What does it feel like?
There’s no single cause of postpartum depression, but physical and emotional issues may play a role.
- Physical changes. After childbirth, a dramatic drop in hormones (estrogen and progesterone) in your body may contribute to postpartum depression. Other hormones produced by your thyroid gland also may drop sharply — which can leave you feeling tired, sluggish and depressed.
- Emotional issues. When you’re sleep deprived and overwhelmed, you may have trouble handling even minor problems. You may be anxious about your ability to care for a newborn. You may feel less attractive, struggle with your sense of identity or feel that you’ve lost control over your life. Any of these issues can contribute to postpartum depression.
Who’s at risk?
Women with a personal or family history of depression or mood or anxiety disorders are more likely to develop PPD, as are those who experience significant mood-related changes related to their menstrual cycles. But perhaps the biggest risk factor is having had PPD with a previous pregnancy—especially if it was untreated.
When to see a doctor
If you’re feeling depressed after your baby’s birth, you may be reluctant or embarrassed to admit it. But if you experience any symptoms of postpartum baby blues or postpartum depression, call your doctor and schedule an appointment. If you have symptoms that suggest you may have postpartum psychosis, get help immediately.
How is it treated?
Treatment and recovery time varies, depending on the severity of your depression and your individual needs. If you have an underactive thyroid or an underlying illness, your doctor may treat those conditions or refer you to the appropriate specialist. Your doctor also may refer you to a mental health provider.
Postpartum depression is often treated with psychotherapy (also called talk therapy or mental health counseling), medication or both.
- Psychotherapy. It may help to talk through your concerns with a psychiatrist, psychologist or another mental health provider. Through therapy, you can find better ways to cope with your feelings, solve problems, set realistic goals and respond to situations in a positive way. Sometimes family or relationship therapy also helps.
- Antidepressants. Your doctor may recommend an antidepressant. If you’re breastfeeding, any medication you take will enter your breast milk. However, some antidepressants can be used during breastfeeding with little risk of side effects for your baby. Work with your doctor to weigh the potential risks and benefits of specific antidepressants.
With appropriate treatment, postpartum depression usually goes away within six months. In some cases, postpartum depression lasts much longer, becoming a chronic depression. It’s important to continue treatment after you begin to feel better. Stopping treatment too early may lead to a relapse.
Helping a friend or loved one
Treatment for postpartum psychosis can challenge a mother’s ability to breastfeed. Separation from the baby makes breastfeeding difficult, and some medications used to treat postpartum psychosis aren’t recommended for women who are breastfeeding. If you’re experiencing postpartum psychosis, your doctor can help you work through these challenges.
People with depression may not recognize or acknowledge that they’re depressed. They may not be aware of signs and symptoms of depression. If you suspect that a friend or loved one has postpartum depression or is developing postpartum psychosis, help them seek medical attention immediately. Don’t wait and hope for improvement.
The information, including but not limited to, text, graphics, images and other material contained on this website are for informational purposes only. The purpose of this website is to promote broad consumer understanding and knowledge of various health topics. It is not intended to be a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or another qualified healthcare provider with any questions you may have regarding a medical condition or treatment and before undertaking a new health care regimen, and never disregard professional medical advice or delay in seeking it because of something you have read on this website.

How to Bond with Your Unborn Baby?
Pregnancy is just the beginning of a life-long love affair with your child. The easy weeks can be tiring and stressful, and it’s easy to feel a bit disconnected from your growing baby. But as your pregnancy progresses, and your bump grows, you’ll start to feel much more like a mom to be.
To help prepare for your new life, spend a little time bonding with your unborn baby when you can. We’ve got some great tips to help you get in touch with this new little person.
Here are 10 things you can try to help you bond with your bump:
- Use Your Voice. When your baby is born, she will recognize your voice and turn towards you whenever she hears it. She will remember your voice because she has spent months listening to you give presentations at work. Spend some time each day talking to your baby, telling her about the things you will do together, touching your belly, reading your favorite childhood book to your baby. You can put headphones on your belly and play music for your baby. You can sing your favorite lullaby. All really great ways to connect with your baby during pregnancy. You may find that your baby responds to the sound of your voice, and begins kicking and nudging you as you talk. If you feel uncomfortable talking to your bump, trying singing instead.

- Go Swimming. Swimming is a great way to take the weight off your feet, and it even gives you some idea of what life is like for your baby! Not only is swimming a safe way to exercise but since your baby’s floating in fluid too, it gives you a chance to relate to her. No matter how big your bump, the gentle support of the water will give you some welcome relief in the later stages of your pregnancy. You could also look out for aquanatal classes. These are an ideal opportunity to tone up and make new friends.
 Massage your Bump. A soothing way to bond with your baby is to gently massage your belly. This is safe to do after the first three months of pregnancy, and it’s a great way to relax and wind down. An aromatherapy massage is a great way to pamper yourself. It gives you a wonderful chance to sit still and spend time thinking of and talking to your baby. Try adding one or two drops of lavender, frankincense or ylang-ylang to a carrier oil for massage. All of these oils are safe to use after the first trimester. Ask your partner if he’d like to give you a massage. It may help him to share in your pregnancy more easily.
Massage your Bump. A soothing way to bond with your baby is to gently massage your belly. This is safe to do after the first three months of pregnancy, and it’s a great way to relax and wind down. An aromatherapy massage is a great way to pamper yourself. It gives you a wonderful chance to sit still and spend time thinking of and talking to your baby. Try adding one or two drops of lavender, frankincense or ylang-ylang to a carrier oil for massage. All of these oils are safe to use after the first trimester. Ask your partner if he’d like to give you a massage. It may help him to share in your pregnancy more easily.

- Nudge Back. For now, your baby’s only method of communication is bumps, kicks, and nudges. You have probably noticed that your baby becomes particularly active when you sit down to rest. Play with your baby by responding to her movements, gently poke back when she nudges you, and see what she does. You can also rub your belly in the area you feel movements.
- Take a Yoga, Classes. Prenatal Yoga classes give you a chance to escape the humdrum of daily life and focus
 on your pregnancy for a while. The yoga teacher will talk you through each pose, explaining how it is beneficial during pregnancy. You will also be given time to relax and focus on your developing baby. This is a great way to guarantee yourself time to focus, which can be difficult to find when you are tying up loose ends at work, packing a hospital bag and preparing the house for a new baby. Yoga has been proven to be beneficial for depression and anxiety during pregnancy.
on your pregnancy for a while. The yoga teacher will talk you through each pose, explaining how it is beneficial during pregnancy. You will also be given time to relax and focus on your developing baby. This is a great way to guarantee yourself time to focus, which can be difficult to find when you are tying up loose ends at work, packing a hospital bag and preparing the house for a new baby. Yoga has been proven to be beneficial for depression and anxiety during pregnancy.

Every pregnancy and every pregnant woman is unique.
- Have a Bath. A nice long soak is a perfect way to get away from it all and enjoy some real “me time”. It’s also a great chance to devote some attention to your baby. Just make sure the water’s not too hot, as this can be bad for your baby. Run a warm bath and perhaps light some candles and play soft music in the background for a soothing ambiance. Then simply lie still, breathe deeply, relax completely and picture your baby. Try taking a few minutes to visualize yourself holding her when she finally arrives. Imagine what she might look like, what you might say to her and how that first cuddle might feel. If you’re well into your second trimester, you may have already felt your baby’s movements. However, these can be easy to miss when you’re busy during the day. A nice quiet bath is a perfect time to focus on your baby’s squirming and kicking. Get to know the pattern of your baby’s movements, and imagine how big and strong she’s getting!
- Get Dad Involved. It’s not just you who wants to develop a lasting bond with your baby – dad-to-be will want a slice of the action too! When you feel the baby kick, place your partner’s hands over your tummy so that he can feel the movements too, and let him respond by rubbing your bump in the same spot. He could even read baby a book or two. You may find that you develop a stronger bond with both the baby and the dad-to-be simply by watching their relationship strengthen.


- Take Bump Photos. Not only will your own photos make a lovely keepsake once the pregnancy is over, but will also help you to focus on your growing baby during pregnancy. Set a time each week to take a photograph of yourself sideways on. As you compare the bump photos from each week, you will be able to see how much your baby is changing and growing during the pregnancy. This visual reminder may help to make the pregnancy seem more real and will give you time to reflect upon the changes occurring. Booking a professional pregnancy photo shoot towards the end of your pregnancy can make you feel special too, where yourself and your partner (or yourself alone) can have some gorgeous moments captured by a professional, that you will no doubt treasure forever.
- Respond to Baby’s Kicks. You may start to feel your baby’s movements from about 18 weeks to 20 weeks if this is your first baby. Feeling your baby move can be wonderfully reassuring after weeks of having no idea what she’s getting up to in there! Responding to your baby’s kicks is about as close as you will get to two-way communication before she’s born. And you can do it at any time, wherever you are. Rub your bump when your baby moves and you may find that she kicks back at you. There’s nothing quite as exciting as feeling your baby respond to your touch for the very first time.
 Go for a Walk. Try taking some time out to bond with your bump by going for a walk. It’s great exercise and easy to fit into your daily routine, even if you’re working. Going for a stroll gives you space to think about your baby without too many distractions or interruptions. You can even have a discreet chat with your bump as you go. If you didn’t do much exercise before you became pregnant, start with a gentle stroll at a pace that’s comfortable for you. Once you’ve got into the habit of walking regularly, you can build up to faster walks lasting between 20 minutes and 30 minutes. You could alternate a few minutes of brisk walking with a few minutes at a slower pace.
Go for a Walk. Try taking some time out to bond with your bump by going for a walk. It’s great exercise and easy to fit into your daily routine, even if you’re working. Going for a stroll gives you space to think about your baby without too many distractions or interruptions. You can even have a discreet chat with your bump as you go. If you didn’t do much exercise before you became pregnant, start with a gentle stroll at a pace that’s comfortable for you. Once you’ve got into the habit of walking regularly, you can build up to faster walks lasting between 20 minutes and 30 minutes. You could alternate a few minutes of brisk walking with a few minutes at a slower pace.

The information, including but not limited to, text, graphics, images and other material contained on this website are for informational purposes only. The purpose of this website is to promote broad consumer understanding and knowledge of various health topics. It is not intended to be a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or another qualified healthcare provider with any questions you may have regarding a medical condition or treatment and before undertaking a new health care regimen, and never disregard professional medical advice or delay in seeking it because of something you have read on this website.

5 Chronic Lung Disease that Often Require Oxygen Therapy
Your lungs have a very important job which is to absorb oxygen from the air and transfer it into your bloodstream, according to the National Heart, Lung and Blood Institute (NHLBI). But some diseases and conditions can keep your body from getting the oxygen it needs. People with chronic diseases have ineffective or heavy breathing pattern 24/7 with deep breathing 24/7. If you develop one of these conditions, and your blood oxygen level falls too low, your doctor may prescribe supplemental oxygen and a finger pulse oximeter to monitor the oxygen level.
Oxygen therapy, also known as supplemental oxygen, is the use of oxygen as a medical treatment. This can include low blood oxygen, carbon monoxide toxicity, cluster headaches, and to maintain enough oxygen while inhaled anesthetics are given. Supplemental oxygen, especially portable oxygen solutions, helps those with chronic lung diseases to enjoy life to the fullest. A portable oxygen unit, like a portable concentrator, can help you regain your independence and mobility while allowing you to increase your physical fitness, as well as time spent with family and friends.
While considering carbon dioxide effects, we also found that chronic overbreathing leads to reduced oxygen transport to cells. As a result, ineffective breathing patterns cause tissue hypoxia, chronic inflammation, immunosuppression, and many other negative effects caused by low body-oxygen levels and hypocapnia (reduced CO2 levels).
Meanwhile, it is known that tissue hypoxia is the driving force of cancer, heart disease, diabetes, chronic fatigue and many other health conditions. Hence, the more people breathe, the more severe health problems, diseases, and symptoms they are going to experience.
The following are Conditions and Diseases that may require supplemental oxygen to help you feel better:
- Cystic Fibrosis. An inherited disease that affects the secretory glands, including those that produce mucus and sweat, according to NHLBI. One of the causes of Cystic Fibrosis is Chronic Hyperventilation. Unfortunately, with CF, thick sticky mucus collects in the airways, creating an ideal place for bacteria to grow. After repeated, intense lung infections, the lungs become severely compromised. Supplemental oxygen can help the lungs do their job.
- Pulmonary fibrosis. A lung disease that occurs when lung tissue becomes damaged and scarred. A person is often diagnosed with pulmonary fibrosis (PF) when tissues in the lungs become thickened, stiff and make it more difficult for your lungs to work properly. As pulmonary fibrosis worsens, you become progressively more short of breath. The Mayo Clinic provides many reasons someone could develop PF, including long-term exposure to occupational toxins, radiation treatment, certain diseases and medical conditions. However, in many cases, the cause remains unknown. As the disease progresses, it decreases the amount of oxygen lungs can transfer to the bloodstream. Supplemental oxygen Helps to reduce breathlessness, while portable solutions enable those with PF to be more physically active.
- Chronic bronchitis: Chronic bronchitis is one type of COPD (chronic obstructive pulmonary disease). This leads to coughing and difficulty breathing. Cigarette smoking is the most common cause. Breathing in air pollution, fumes, or dust over a long period of time may also cause it. The disease, which will get worse over time, is characterized by a constant cough and a large amount of mucus. When caught early, the disease can then be managed so you can live a full, active life. As the disease progresses, portable oxygen solutions can allow you the mobility and independence you need to get out and moving more often.
- Emphysema: a condition in which the small air sacs of the lungs are damaged and enlarged, causing breathlessness. The No. 1 culprit of an emphysema diagnosis is smoking. This disease makes it harder and harder to breathe normally. Those with emphysema often become short of breath on a regular basis. However, supplemental oxygen can help provide some relief by increasing blood oxygen levels and making oxygen distribution easier on the body.
- Alpha 1 Antitrypsin Deficiency: An inherited disorder that may cause lung disease and liver disease. This genetic disorder can lead to breathing problems at a young age and eventually develop into emphysema or Chronic Obstructive Pulmonary Disease (COPD), according to WebMD. The Alpha 1 Antitrypsin enzyme is found in the lungs and bloodstream and is meant to prevent inflammation and its effects in the lungs. When your body lacks enough of this enzyme, it can lead to emphysema and make it difficult to breathe. NHLBI says supplemental oxygen, along with bronchodilators and pulmonary rehabilitation, are common treatments of AAT deficiency.
The critical oxygen level is an oxygen saturation of approximately 90% (this is measured by a finger pulse oximeter), equivalent to a blood oxygen level of 55-60 mmHg (this is measured from a blood sample taken from an artery, commonly in the wrist). This blood test is known as an arterial blood gas or ABG. Therefore, controlled oxygen therapy, to maintain oxygen saturation at around 90% (88-92% is an acceptable range). It is important to avoid too much oxygen and minimize the risk of worsening CO2 levels in this situation. Some patients who are very sensitive to the adverse effects of too much oxygen may choose to wear a medical alert bracelet to alert paramedics about their lung condition in the event of an emergency.
The information, including but not limited to, text, graphics, images and other material contained on this website are for informational purposes only. The purpose of this website is to promote broad consumer understanding and knowledge of various health topics. It is not intended to be a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or another qualified healthcare provider with any questions you may have regarding a medical condition or treatment and before undertaking a new health care regimen, and never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Resources:
http://www.domorewithoxygen.com/bid/293363/5-chronic-lung-diseases-that-often-require-oxygen-therapy

Calcium During Pregnancy
When you’re pregnant, your developing baby needs calcium to build strong bones and teeth. Calcium also helps your baby grow a healthy heart, nerves, and muscles as well as develop a normal heart rhythm and blood-clotting abilities.
Your body will do whatever it needs to take care of your baby, including stealing. Your body actually takes calcium from your own bones or teeth to give it to your little one. So if you want your bones and teeth to stay strong, you need to get extra calcium while your baby’s growing inside you.
What Calcium Does for You
It’s common knowledge that calcium is crucial for proper fetal bone and teeth development. But were you aware that you and your baby need calcium to maintain a normal heartbeat? Besides building teeth and bones, calcium also keeps your blood and muscles moving and helps your nerves send messages from your brain to the rest of your body.
Calcium You Need During Pregnancy
Your body can’t make calcium, so you need to get it from food or supplements. While you’re pregnant, try to get at least 1,000 mg of calcium every day. If you’re 18 or younger, then you need at least 1,300 mg of calcium every day.
Dietary sources of calcium 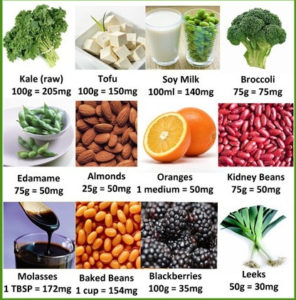
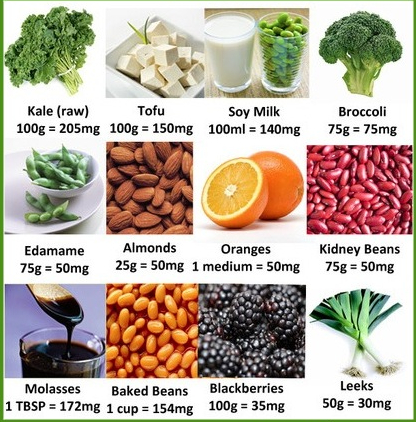
- Yogurt, 8 oz, plain low-fat: 415 mg
- Orange juice, 6 oz of calcium-fortified OJ: 375 mg
- Sardines, 3 oz canned with bones in oil: 325 mg
- Cheddar cheese, 1.5 oz: 307 mg
- Milk, 8 oz nonfat: 299 mg
- Tofu, 1/2 cup, firm, made with calcium sulfate: 253 mg
- Salmon, 3 oz canned with bones: 181 mg
- Cereal, 1 cup of calcium-fortified types : 100 to 1,000 mg
- Kale, 1 cup, cooked: 94 mg
- Soy beverage, 8 oz, calcium-fortified: 80 to 500 mg:
- Bok choy, 1 cup, raw: 74 mg
Here are a few examples on how to reach that 1,000 mg goal: Drink 3 cups of milk or calcium-fortified orange juice or choose a cereal that has 1,000 mg of calcium.
Know About Calcium Supplements
 Whether you were calcium deficient prior to pregnancy and if you’re having trouble meeting your RNI with food alone. Before popping calcium pills, make sure to talk to your GP first and have a dietitian review your current diet.
Whether you were calcium deficient prior to pregnancy and if you’re having trouble meeting your RNI with food alone. Before popping calcium pills, make sure to talk to your GP first and have a dietitian review your current diet.
An excessive calcium intake (from supplements) can harm your baby: some babies fail to thrive, while others suffer from various symptoms ranging from mild constipation, muscle weakness to severe seizures. According to studies, excess calcium intake can also hinder the absorption of other minerals such as iron, magnesium, and zinc which are also essential for both mother and child.
Calcium supplements come in two forms: carbonate and citrate.
- Calcium carbonate is less expensive and works best if you take it with food.
- Calcium citrate works just as well with food or on an empty stomach.
Many calcium supplements also contain vitamins D, which helps your body absorb calcium.
Limit to 500 mg at a time. To make sure your body absorbs the most calcium possible, take only 500 mg of calcium at a time. For example, this might mean taking a 500 mg supplement with breakfast and another with dinner.
The information, including but not limited to, text, graphics, images and other material contained on this website are for informational purposes only. The purpose of this website is to promote broad consumer understanding and knowledge of various health topics. It is not intended to be a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or another qualified healthcare provider with any questions you may have regarding a medical condition or treatment and before undertaking a new health care regimen, and never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Resources:
https://www.webmd.com/baby/get-the-calcium-you-need-during-pregnancy#1

Multiple Pregnancy
A multiple pregnancy is when you are pregnant with twins, triplets or more. Three babies or more is called a ‘higher order’ pregnancy, and it’s rare – occurring in just 1 in 50 multiple pregnancies.
Having twins, triplets or more can be challenging, but most families find having several babies at once a positive experience.
How does multiple pregnancy occur? 

Multiple pregnancies occur when more than one embryo implants in your uterus (womb). This can happen if you release more than one egg during the menstrual cycle and each egg is fertilized by a sperm. Sometimes, a fertilized egg spontaneously splits into 2, resulting in identical embryos. This type of pregnancy results in fraternal twins (or more). When a single fertilized egg splits, it results in multiple identical embryos. This type of pregnancy results in identical twins (or more). Identical twins are less common than fraternal twins.
What are some causes of multiple pregnancy?
The use of fertility drugs to induce ovulation often causes more than one egg to be released from the ovaries and can result in twins, triplets, or more. Multiple pregnancies are more common than they used to be, mainly because of the increasing use of in vitro fertilization (IVF) if more than one embryo is transferred to the uterus. Identical multiples also may result if the fertilized egg splits after transfer. Women aged 35 and older are more likely to release more than one egg during ovulation, so they are more likely to have a multiple pregnancy. You are also more likely to have a multiple pregnancy if you have a history of twins in your family.
What are some symptoms of multiple pregnancy?
Women who are pregnant with multiples may have more severe morning sickness or breast tenderness than women who are pregnant with a single baby. They also may gain weight more quickly. A multiple pregnancy is confirmed by an ultrasound scan, usually in the first trimester (the first 12 weeks). The ultrasound will confirm the type of multiple pregnancy, whether there is one placenta or 2, and how many amniotic sacs there are. These are all important factors for later in the pregnancy and it’s important to identify them as early as possible.
Types of multiple pregnancy
Fraternal twins 

Two separate eggs are fertilized and implant in the uterus. The babies are siblings who share the same uterus – they may look similar or different, and may either be the same gender (2 girls or 2 boys) or of different genders. A pregnancy with fraternal twins is statistically the lowest risk of all multiple pregnancies since each baby has its own placenta and amniotic sac. You will sometimes hear fraternal twins referred to as ‘dizygotic’ twins, referring to 2 zygotes (fertilized eggs).
Identical twins
 Identical twins are formed when a single fertilized egg is split in half. Each half (embryo) is genetically identical, so the babies share the same DNA. That means the babies will share many characteristics. However, because their appearance is influenced by the environment as well as by genes, sometimes identical twins can look quite different. Identical twins may share the same placenta and amniotic sac, or they may have their own placenta and amniotic sac. You will sometimes hear identical twins referred to as ‘monozygotic’, referring to one zygote (fertilized egg).
Identical twins are formed when a single fertilized egg is split in half. Each half (embryo) is genetically identical, so the babies share the same DNA. That means the babies will share many characteristics. However, because their appearance is influenced by the environment as well as by genes, sometimes identical twins can look quite different. Identical twins may share the same placenta and amniotic sac, or they may have their own placenta and amniotic sac. You will sometimes hear identical twins referred to as ‘monozygotic’, referring to one zygote (fertilized egg).
Triplets and ‘higher order multiples’ (HOMs)
Triplets, quadruplets, quintuplets, sextuplets or more can be a combination both of identical and fraternal multiples. For example, triplets can be either fraternal (trizygotic), forming from 3 individual eggs that are fertilized and implanted in the uterus; or they can be identical, when one egg divides into 3 embryos; or they can be a combination of both.
Do I need to gain extra weight if I am pregnant with multiples?
It generally is recommended that women who are pregnant with multiples gain more weight than women who are pregnant with one baby. An extra 300 calories a day is needed for each fetus. For instance, if you are pregnant with twins, you need an extra 600 calories a day. For triplets and higher-order pregnancies, weight gain should be individualized.
Complications of Multiple Pregnancy
The most common complications include the following: 
- Preterm labor and birth. Over 60% of twins and nearly all higher-order multiples are premature (born before 37 weeks). The higher the number of fetuses in the pregnancy, the greater the risk for early birth. Premature babies are born before their bodies and organ systems have completely matured. These babies are often small, with low birth weights (less than 2,500 grams or 5.5 pounds), and they may need help breathing, eating, fighting infection, and staying warm. Very premature babies, those born before 28 weeks, are especially vulnerable. Many of their organs may not be ready for life outside the mother’s uterus and may be too immature to function well. Many multiple birth babies will need care in a neonatal intensive care unit (NICU).
- Gestational hypertension. Women with multiple fetuses are more than twice as likely to develop high blood pressure of pregnancy. This condition often develops earlier and is more severe than pregnancy with one baby. It can also increase the chance of placental abruption (early detachment of the placenta).
- Anemia. Anemia is more than twice as common in multiple pregnancies as in a single birth.
- Birth defects. Multiple birth babies have about twice the risk of congenital (present at birth) abnormalities including neural tube defects (like spina bifida), gastrointestinal, and heart abnormalities.
- Miscarriage. A phenomenon called the vanishing twin syndrome in which more than 1 fetus is diagnosed, but vanishes (or is miscarried), usually in the first trimester, is more likely in multiple pregnancies. This may or may not be accompanied by bleeding. The risk of pregnancy loss is increased in later trimesters as well.
- Twin-to-twin transfusion syndrome. Twin-to-twin transfusion syndrome (TTTS) is a condition of the placenta that develops only with identical twins that share a placenta. Blood vessels connect within the placenta and divert blood from one fetus to the other. It happens in about 15% of twins with a shared placenta.
In TTTS, blood is shunted from 1 fetus to the other through blood vessel connections in a shared placenta. Over time, the recipient fetus receives too much blood. This can overload the cardiovascular system and cause too much amniotic fluid to develop. The smaller donor fetus does not get enough blood and has low amounts of amniotic fluid. TTTS can be treated during pregnancy by withdrawing some of the extra fluid with a needle or with surgery on the placenta. Sometimes, the twins may need to be delivered early.
- Cerebral Palsy: A long-term disability of the nervous system that affects young children in which control of movement or posture is abnormal and is not the result of a recognized disease.
- Abnormal amounts of amniotic fluid. Amniotic fluid abnormalities are more common in multiple pregnancies, especially for twins that share a placenta.
- Cord entanglement. Cord entanglement for the twins that share the amniotic sac. In these cases, monitoring of the fetuses often in the third trimester may be necessary.
- Cesarean delivery. Abnormal fetal positions increase the chances of cesarean birth.
- Postpartum hemorrhage. The large placental area and over-distended uterus place a mother at risk for bleeding after delivery in many multiple pregnancies.
Can multiple pregnancy affect my risk of postpartum depression? 

Multiple births increase the risk of postpartum depression. Multiple births are a risk factor for postpartum depressive symptoms in mothers. If you have intense feelings of sadness, anxiety, or despair that prevent you from being able to do your daily tasks, let your obstetrician or other members of your health care team know.
Can I breastfeed if I have multiples?
Yes, but it may take some practice. Your milk supply will increase the right amount. You will need to eat healthy foods and drink plenty of liquids. The law of supply and demand applies to nursing mothers of twins and multiples. If you breastfeed when your babies want to eat, you can trust your body to supply enough milk. A low milk supply can almost always be corrected by nursing more often. If your babies aren’t emptying your breasts, you may need to pump.
The information, including but not limited to, text, graphics, images and other material contained on this website are for informational purposes only. The purpose of this website is to promote broad consumer understanding and knowledge of various health topics. It is not intended to be a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or another qualified healthcare provider with any questions you may have regarding a medical condition or treatment and before undertaking a new health care regimen, and never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Resources:

How to Have a Smart Baby
Living a healthy lifestyle while you’re expecting helps your baby grow big and strong, but did you know it can make her smarter too? In fact, simple choices that you make every day, from eating a leafy-green salad for lunch to hitting the treadmill for a workout, can help build her brain. What you do while you’re pregnant can have as much impact on your child’s brain development and future intelligence as what you do after you give birth and taking care of yourself now will help prepare your baby to be an active learner.
Lowered Autism Odds:
Pop Your Prenatal Vitamin Daily
Taking it will help ensure that you get the balance of nutrients your baby needs, like folic acid and vitamin B12 to make red blood cells, vitamin C to produce collagen, vitamin D for bone building, and zinc for brain development. If your vitamin upsets your stomach, don’t just ditch it: Try taking it with a meal, or talk to your doctor about switching brands.
Get Omega-3s

Fish, rich in omega-3 fatty acids, may boost your baby’s brain power. In a study from Harvard Medical School, the more fish women ate during the second trimester, the higher their babies scored on a mental-development test at 6 months of age. Omega-3s are found in brain-cell membranes, so there are plenty of ways they can influence brain function, says Lisa Eliot, Ph.D., assistant professor at Rosalind Franklin University of Medicine and Science, in Chicago. If you don’t like fish, talk to your doctor about taking a fish-oil supplement.
Pump Up Iron
 Your iron intake needs to double during pregnancy since iron helps deliver life-sustaining oxygen to your baby. Iron helps promote the growth of healthy red blood cells, which carry oxygen to your baby’s brain. Trouble is, many women enter pregnancy already deficient, says Somer. If your baby’s deprived of oxygen in the womb, the risk of poor growth — and lower IQ — increases. Ask your doctor to test you for iron deficiency. Then make sure your diet includes iron-rich foods like lean beef, chicken, legumes, beans, spinach, tofu and as well as iron-enhanced cereals.
Your iron intake needs to double during pregnancy since iron helps deliver life-sustaining oxygen to your baby. Iron helps promote the growth of healthy red blood cells, which carry oxygen to your baby’s brain. Trouble is, many women enter pregnancy already deficient, says Somer. If your baby’s deprived of oxygen in the womb, the risk of poor growth — and lower IQ — increases. Ask your doctor to test you for iron deficiency. Then make sure your diet includes iron-rich foods like lean beef, chicken, legumes, beans, spinach, tofu and as well as iron-enhanced cereals.
Increased Intelligence:
Working out will give you the stamina you need for labor and delivery, and it can also strengthen your baby’s brain. According to a study in the Journal of the American College of Sports Medicine, children of moms who exercised during pregnancy scored higher on tests of language skills and intelligence at age 5 compared with the kids of sedentary moms. Why? Moderate levels of cortisol — a stress hormone that’s also secreted when you exercise — promote the growth and development of your baby’s brain, as well as his other major organs. Experts recommend 30 minutes of moderate exercise for pregnant women on all or most days of the week.
Maximum Brainpower:
Fetal Brain Development
The fetal brain goes through several stages of development. During the first trimester, the nerve cells form but are not actually developed as a brain. Impulses begin to fire without pattern or direction. Sensory organs and nerves are not developed at this point, so the fetus does not feel pain. During this time, it’s especially important to avoid chemicals and dangerous substances. The first trimester is a time of exponential growth.
During the second trimester, nerve functions start to synchronize and differentiate. The sensory organ begins development, as do the nerves. About the 5th month, the baby can now start to feel, although the sensations they feel are very limited and erratic. Those healthy fats provide faster development and healthier nerve connections.
During the last trimester, the brain is forming learning abilities and beginning memories. This is a time where exposure to classical music and soothing sounds will affect the child’s disposition later in life.
Be Mindful of Mercury
Fish is good for your baby’s brain, but you do need to take a few precautions. Mercury contamination in some fish may be harmful. The Food and Drug Administration advises all pregnant women to avoid shark, tilefish, king mackerel, and swordfish completely since they contain the highest levels. Some lower-mercury options: salmon, catfish, pollack, whitefish, tilapia, and shrimp. Even with these varieties, you should limit all fish to 12 ounces (about two meals) per week. And opt for canned light tuna over canned white albacore, which has more mercury.
Munch on Fruits and Veggies 
Produce contains antioxidants, which are good for your baby. “Antioxidants protect the baby’s brain tissue from damage,” says nutritionist Elizabeth Somer, RD, author of Nutrition for a Healthy Pregnancy. Choose deep-colored produce — like dark leafy greens, papaya, blueberries, and tomatoes — for the biggest antioxidant punch. Regular consumption of fruit is known to reduce a variety of health complications such as Alzheimer’s or preventing weight gain but now new research has suggested that we may benefit from a diet high in fruit earlier than we thought.
Child development experts in Canada found that women who eat fruit during their pregnancy are more likely to give birth to smarter children than those who do not or eat very little fruit.
Avoid Alcohol
Though fetal alcohol syndrome is associated with heavy alcohol abuse during pregnancy, even moderate amounts of beer, wine, or liquor can harm a baby’s brain, according to the March of Dimes. Light to moderate drinking can lead to problems with learning, attention, memory, and social skills down the road.
Don’t Gain Too Much
You’re eating for two now, but packing on too many pounds during pregnancy ups your chances of a premature delivery — and babies born early may be at a disadvantage when it comes to learning. “Premature delivery is one of the greatest risk factors for mental impairment,” says Dr. Lise Eliot. “There’s a strong link between birth weight, IQ score, and school achievement.” What’s the connection? Babies born early miss out on the unique nourishment that the placenta provides, are exposed to stimuli they’re normally protected from in the womb and are more vulnerable to infection. To keep your weight healthy, follow these guidelines:
- If you’re currently a normal weight, gain 25-35 pounds.
- f you’re currently overweight, gain 15-25 pounds.
- If you’re currently underweight, gain 28-40 pounds.
Your baby’s brain will develop through various experiences and exercises. Senses of touch, smell, sight, sound, and taste will also aid this development process. You need to start giving your baby different sensory experiences from an early age, to help him identify and differentiate things. Development of his cognitive and motor skills will help you know how to raise a smart baby.
The information, including but not limited to, text, graphics, images and other material contained on this website are for informational purposes only. The purpose of this website is to promote broad consumer understanding and knowledge of various health topics. It is not intended to be a substitute for professional medical advice, diagnosis or treatment. Always seek the advice of your physician or another qualified healthcare provider with any questions you may have regarding a medical condition or treatment and before undertaking a new health care regimen, and never disregard professional medical advice or delay in seeking it because of something you have read on this website.
Resources:
https://www.parents.com/pregnancy/my-baby/how-to-have-a-smart-baby-pregnancy-brain-power-boosters/